Recurrence Rate of Small Melanoma In Situ on Low-Risk Sites Excised With 5-mm Excisional Margin
Published:
09/20/2024

How much is enough?
Exploring excisional margins for in situ melanoma
When a patient with melanoma in situ has a wide local excision, the clinician will remove the entire melanoma as well as extra, healthy skin surrounding the melanoma in situ. The goal is to get what is called “clear margins,” which means no cancer cells are visible at the edge of the tissue, an indication that all the cancer has been removed. The ultimate goal is to prevent, as much as possible, the recurrence of the cancer.
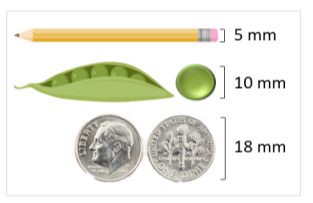
However, there are variations among clinical recommendations about the standard for clear margins. In other words, there is some disagreement on how much healthy skin should be removed around a lesion. The guidelines throughout the world vary, with some countries, like the U.S. and Australia, suggesting 5-10 mm and others, like South Africa, suggesting 18 mm for the treatment of lentigo maligna. A recent study explored the question – how wide should the margins be for a melanoma in situ lesion?
A private practice in Australia analyzed data from 351 melanoma in situs from 292 patients in order to answer this question. A total of 345 lesions had clear margins after initial wide local excision with 5 mm margins and six patients required more tissue to be removed in order to achieve clear margins.
 Out of the 351 melanoma in situs, 348 had no documented recurrence of melanoma in situ after seven years. Only three recurred, and these were observed locally within the prior scar of the excision. The data means that 99.1% of the melanoma in situs did not recur.
Out of the 351 melanoma in situs, 348 had no documented recurrence of melanoma in situ after seven years. Only three recurred, and these were observed locally within the prior scar of the excision. The data means that 99.1% of the melanoma in situs did not recur.
The study is important because it demonstrates how much tissue is enough to remove around an in situ lesion to reasonably guarantee there will not be a recurrence. Although these sizes look negligible to the human eye, there is a vast difference on the microscopic level. Several million cells exist in each millimeter of tissue, so a billion cells could be impacted in each patient with even a slight change in the guidelines. With the number of cases of melanoma in situ increasing annually, the study could impact thousands of patients who have a wide local excision.
Dr. Wesley Yu, MD, Associate Professor, and Mohs Surgeon at the Oregon Health and Science University said, “This study is important because it points to the possibility of narrowing surgical margins for patients with small melanomas on low-risk sites.” Reducing the margin size could also improve the quality of life for patients, particularly those with lesions on the face, head, and neck. “The data need to be interpreted carefully since this was a retrospective study with exclusion criteria that could have introduced bias. However, overall this study is very suggestive, important, and further supports the need for prospective clinical trials to determine the best surgical treatments for melanoma,” Dr. Yu said.
This summary is based on the report by Sun C et al. Recurrence Rate of Small Melanoma In Situ on Low-Risk Sites Excised With 5-mm Excisional Margin. JAMA Dermatol. 2024 Aug 1;160(8):874-877.
Recent Posts

Apr. 28, 2025
Your Style Can Save Lives – Lilly Pulitzer Giving Day is Here!

Apr. 28, 2025
From Diagnosis to Crown: Miss Pennsylvania’s Journey of Advocacy and Awareness

Apr. 24, 2025
Worried Your Melanoma Treatment Isn’t Working?

Apr. 24, 2025
Genetic Testing Performed in Melanoma

Apr. 16, 2025